Hello everyone,
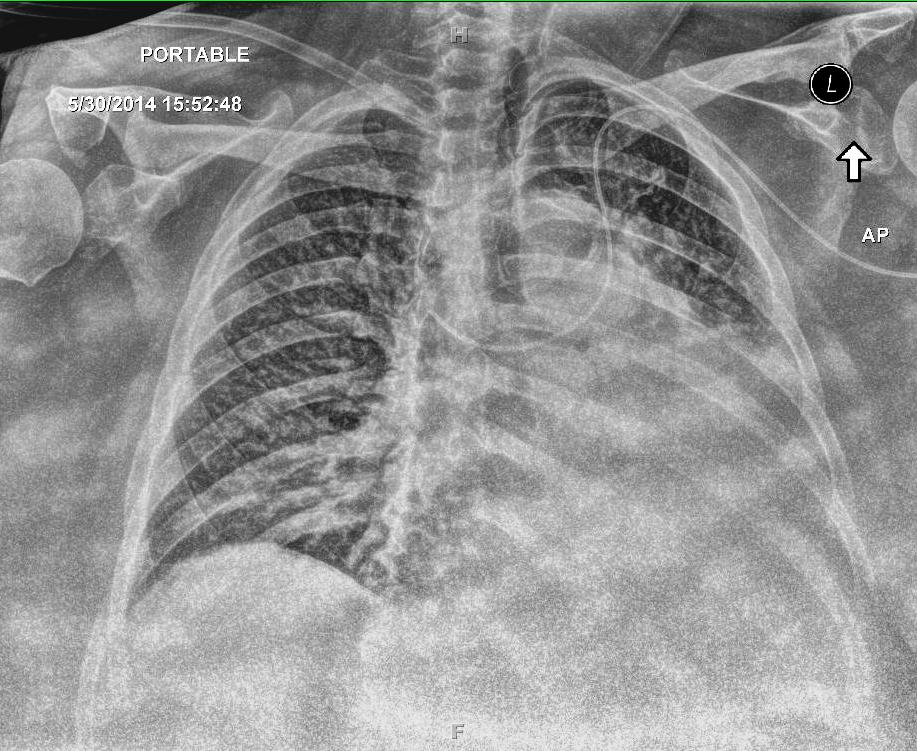
I placed a PICC in a morbidly obese female last week. I've attached the Chest X-ray for your review. I would like to know if anyone has seen this before? One radiologist recommended repositioning the line. This is not a left sided SVC. Another one I spoke with stated he would leave it in place as is, because it would be difficult to reposition and it is in the central circulation. The patient will need 14 days of Ceftriaxone IV. And the PICC was trimmed at 57 cm.
Would like to know your thoughts. Thanks!
Ann Armstrong, RN
MMC Midland, MI
| Attachment | Size |
|---|---|
| 138.87 KB |
{kind=link}
How do you know this is not a left SVC? It has definitely taken an aberrant path into some unconfirmed location, which could easily be a smaller tributary vein or the coronary sinus. So it needs to be repostioned in my opinion. It there is a serious complication and a lawsuit results (not saying it will but anything is possible), this xray would be strong evidence for the plaintiff (patient). With a radiology recommendation to reposition and you choose not to do it, again there would not be any likely defense for that action. Lynn
Lynn Hadaway, M.Ed., RN, CRNI
Lynn Hadaway Associates, Inc.
PO Box 10
Milner, GA 30257
Website http://www.hadawayassociates.com
Office Phone 770-358-7861
Wow that's impressive. Thanks for sharing this.
Ceftriaxone is 'Administration: Injectable Detail pH: 6.6 (premixed infusion solution); 6.7 (1% aqueous solution)', which is not to irritating. In fact it can be administered IM. Have you considered a midline, used NTE 28days? The midline would not be centrally placed, so the right v. left issues of central vasculature can be avoided. Also, larger peeps often have v. large cephalic veins. Good luck, keep us updated!
Is there a prior chest ct scan? That could shed some light. If looks like a low hanging left brachiocephalic. I don't believe the left internal thoracic takes that medial path. The left internal thoracic can mimic left SVC or aortic placement.
Why did you go on the left?
Darilyn
Ann Armstrong, RN
PICC Lines
MidMichigan Medical Center, Midland
Hi Darilyn,
I went on the left because this very large lady was situated on the left side of the bariatric triflex bed.
Ann
Ann Armstrong, RN
PICC Lines
MidMichigan Medical Center, Midland
IMO, it needs to be removed. Rule #1 is Do No Harm, especially if there are better options available. Which would be to probably have IR place a new picc under fluoro.
It's def an odd path, almost looks like it needs more length to turn the final corner down. I've placed some piccs where the line on the cxr resembles a set of stairs.
Regardless, though, even if you were sure it was in the svc, the tip is completely sideways, even pointing up a bit, which is not good for the patient, higher risk of vessel wall injury/thrombosis/etc. If this line was in me and I saw the xray, I would politely request it be removed immediately. That's the guideline I try to use when deciding what to do in certain situations...."would I be ok with this line in MY body?"
Did you use tip location system? Ecg or doppler technology?
Sam
I would probably want to investigate a little further. If it flushes and draws with dark venous blood I would first reposition the patient and get another picture, perhaps an oblique too. At times it's just tough to know how to proceed. Like someone else already asked - why the left approach?
Hello Ann-
I agree this is likely a low left brachiocephalic connection to the SVC , although left SVC is also possible - review of previous imaging studies may provide more information. Either way the current position (tip directed across midline and then cephalad) is not acceptable as it increases catheter related risks (vessel irrritation or damage/thrombus/further malposition). Additional length would likely allow optimal (safer) SVC positioning, though the carina and cardiac silhouette are not readily visible in this image. I would agree with removal/replacement and use of fluoroscopic guidance if insertion was difficult or navigation is not available.
I also wonder why the left arm was chosen; whether tip navigation was available/used; what was the original length - would there have been enough if not trimmed and how do you know it's not a left SVC?
Anatomical variations are more prevalent than often realized, I have assisted with or circulated for many PICC/PORT or PPM insertions prior to the VAT creation at our facility. I have also had a couple lines drop left of midline, with radiology read as possible arterial placement. In my cases (lung CA & pleural effusion), the lline traveled subclavicular, dropped on the left, crossed midline and then directed caudally with a left curve on XR. Venous placement was confirmed by running a hemeoximetry on a sample aspirated from the PICC line.
Keely
Keely Ralston RN-BC, VA-BC, CPUI, RCIS
FYI, There is a good article in JAVA this month on patent Left SVC.
Many of you have asked why a PICC was inserted through the left arm. My question is why not use the left arm? I know that many of you will quote some literature on vein thrombosis being greater from the left, etc. But you also must consider ALL factors including hand dominance, especially when the patient is planned for discharge into home care. They will use their dominant hand to attach the syringes and sets so the nondominant hand, most often the left, is needed to hold the catheter hub. There are numerous other reasons for why the left may be the most appropriate extremity for a PICC insertion. So any fear of thrombosis could be managed in other ways - smaller diameter catheters, proper CAJ tip location, adequate hydration, systemic anticoagulation for hypercoagulant patients. Lynn
Lynn Hadaway, M.Ed., RN, CRNI
Lynn Hadaway Associates, Inc.
PO Box 10
Milner, GA 30257
Website http://www.hadawayassociates.com
Office Phone 770-358-7861
To be clear Ann I wasn't questioning your decision to use the left side, there wasn't anything visible to me on the xray prompting a left approach. Right side insertions are my first choice because they are usually shorter and easier placement, but obviously not always possible or best. I'm sure you assessed the patient and the situation just fine. So, what happened? Did the line get a replacement or reposition? Did the patient do OK? Are you comfortable with the outcome?
Thank you Ann for sharing the xray and the situation, I always learn so much from these cases.
Bradford A. Dungan
who had a left-sided triple lumen PICC in place for 4 days, then boom his Xray looks just like this one morning.
It is a left PICC that has flipped its tip upwards. You could try a power flush, but if you cannot get the tip down again, you must reposition. I love the gentle curves that make it so much more interesting, rather than an obvious path throughout the vasculature.
Kathleen Crowe RN CRNI